



The Dreadful Headache, IVIG and Infusion Rates
Dr. Carolina Barnett-Tapia
MD, PhD
2012

Intravenous immunoglobulin (IVIG) remains the first line treatment option for people with CIDP. While the rate of severe adverse events is low, up to 3 in 10 people experience headache, chills, fever and rash, that while not dangerous can be quite severe, and sometimes disabling. Most of these adverse events occur during the infusion, and we have known for several years that many of these are related to the infusion rate (i.e. how fast the infusion is given).
So, what is the “optimal” infusion rate? Well, it depends. Some people have a high tolerance of IVIG and never develop these symptoms and can have fast infusions. Some people develop symptoms even with slow rates. So the optimal rate is the one that works best for an individual. Some people simply cannot tolerate IVIG regardless of the infusion rate and, fortunately, other options, such as subcutaneous Ig are now available.
How do we calculate rates? Well, to make thing trickier, infusion rates are calculated based on weight; remember that the dosing of IVIG is by weight so the rates take this into consideration. Different formulations have different manufacturer’s indications regarding rates, but most have a maximum rate, usually around 0.08 mL/Kg/min. Using this rate, as an example, a person who weighs 70 Kg could receive a maximum rate of 5.6 mL per minute, which is approximately 336 mL per hour. This maximum rate comes from older studies and older formulations which may have had more potential for adverse reactions.
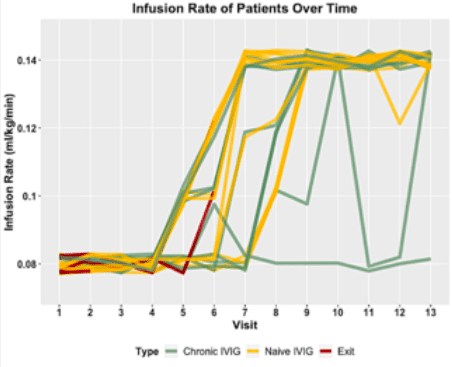
We recently conducted a study to test whether this maximum rate number could be safely exceeded. We enrolled 25 patients with known CIDP attending our clinic. They could be new to IVIG or be on chronic treatment. We planned 13 IVIG (10%) infusions, starting with a low infusion rate on day one, increasing only if tolerated, with a maximum of 0.08 mL/Kg/min. After several infusions, we slowly increased the maximum rate according to tolerance to 0.1, 0.12 and finally to a maximum study rate of 0.14 mL/Kg/min. Using the same example as above—a person who weighs 70K, this would be a maximum rate of 9.8 mL/min or 588 mL per hour.
What did we find? Well, 19 (76%) of the patients were able to safely increase the rate to our maximum study rate. Of these 19 individuals, 2 had some adverse events at the highest rate, and needed to go to a lower rate, but on subsequent infusions, they were able to tolerate the higher rate. Overall, the patients who were able to receive the highest infusion rate were able to reduce their total infusion time by 23%.
What about the patients who did not reach a higher rate? One of them had to use a low rate for all the study infusions. Four patients withdrew from the study altogether, only 2 (8% of total patients) due to adverse events. Of note, the 2 patients who had adverse reactions to IVIG had it after a loading dose (2g/k) given at slow infusion rates. So we think in these specific cases it was not the infusion rate but maybe the amount of fluid or the higher total dose that was problematic.
In our study, we analysed 264 infusions, and we only had 25 treatment-related adverse events, 7 were rash/hives (28%), and 6 (24%) were headaches. We did however -pre- medicate all our patients with acetaminophen and diphenhydramine (anti-allergic), which can help prevent or reduce headache, rash and other adverse events. We also excluded people who had a history of severe reactions to IVIG.
So, what is our current practice? We always recommend to start with a low infusion rate, especially in people new to IVIG. The rate can be then increased slowly (after 30 minutes in the first infusion), according to tolerance. If symptoms develop, the
infusion is slowed down or stopped, and restarted at a lower rate. Sometimes a patient is able to tolerate a higher rate in a future
infusion, so if they are doing well we might re-challenge them if they want to try. The key is to do this slowly and to individualize the rate for the patient. Some patients may always need a low rate even if they don’t develop headache or rash, for example people with acute kidney failure due to higher risk of blood clots (thrombosis).
Some patients develop intolerable symptoms despite good hydration and premedication. Some of these patients may find that a different IVIG formulation is better tolerated. If this does not help or is not feasible, then other treatment alternatives should be considered, such as subcutaneous infusions.
Many hospitals have infusion rate tables, which help infusion nurses to safely increase the rate according to weight, tolerance and to specific formulations. Remember to discuss with your care team if you find that your rate is too fast for you, or if you think you could safely tolerate a higher rate.
References:
1. Hughes RAC, Donofrio P, Bril V, et al. Intravenous immune globulin (10% caprylate- chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): a randomised placebo-controlled trial. Lancet Neurol. 2008;7:136-144.
2. Jiang Y, Mendoza M, Sarpong E et al. Efficacy and safety of high infusion rate IVIG in CIDP. Muscle & Nerve. 2020;62:637-641.
3. Grillo JA, Gorson KC, Ropper AH, Lewis J, Weinstein R. Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders. Neurology. 2001;57:1699-1701
4. Cherin P, Marie I, Michallet M, et al. Management of adverse events in the treatment of patients with immunoglobulin therapy: a review of evidence. Autoimmune Rev. 2016;15:71-81. https://doi.org/10. 1016/j.autrev.2015.09.002

More Medical articles
Learn from the Experts!
In these educational sessions, a wide range of doctors, specialists, therapists and other experts share in depth advice and information.
Watch The Videos